Case story. M. Brivio, MD
Bergamo Hospital, Italy
Endotoxin (or lipopolysaccharide, LPS) is the toxic part of gram-negative bacteria, present in the outer membrane of the bacteria cell wall, released when the bacterial cell disintegrates. High levels of endotoxin activity are associated with worse clinical outcomes and death. 1 Endotoxin is the initial trigger of the inflammatory cascade and is well known to induce direct damage and cause release of inflammatory mediators, potentially leading to sepsis and septic shock. 2
In 2020, the number of sepsis cases was estimated to be 49 million, resulting in 11 million deaths, or 1 in 5 globally. This makes sepsis one of the most common causes of death in modern intensive care with a mortality ranging from 20-50%.
3,4 In addition, 45-70% of acute kidney injury (AKI) cases in the intensive care unit is associated with sepsis.
5
We used an endotoxin removal device (Alteco LPS Adsorber, Lund, Sweden) for extracorporeal blood purification in combination with continuous renal replacement therapy (continuous veno-venous hemodiafiltration, CVVHDF) as an addition to the etiological antibiotic therapy.
Almost all parameters recorded were improved, in particular we could quickly stop vasopressor support and a hemodynamic stability was seen directly after the treatment as well as 12 hours later. The patient was still alive 28 days after the Alteco LPS Adsorber treatment and stayed in total 47 days in ICU after the completion of endotoxin removal. The product was considered safe to use as no device failure occurred, nor side effects or any adverse events.
Case report
A 58-year old male, previously hospitalized in our ICU for COVID-19 pneumonia, was readmitted in ICU with septic shock originating from an E. Coli pyelonephritis. The patient suffered a profound hypotension despite high vasopressors and inotropes dosages.
Method
Treatment with the Alteco LPS Adsorber was started 24 hours after admission, it was continued together with CVVHDF therapy. Two endotoxin removal treatments were performed in a 24-hour period, each one lasting 6 hours.
The following CRRT setting parameters were used: blood flow rate 150 ml/min, dialysate pump flow rate 1500 ml/h and re-infusion pump flow rate 1000 ml/h. Anticoagulation was achieved via a heparin continuous infusion with a 200 seconds activated clotting time (ACT) target.
Vital signs, blood chemistry values, urine output, blood gas analysis, hemodynamic parameters, SOFA score, inotropes and vasopressor dosages were recorded right before the first treatment start, at the end of the treatments and 12 hours after treatments ended.
Results
Hemodynamic parameters did improve during treatment: vasopressor support was reduced and norepinephrine was discontinued; cardiac index, systemic vascular resistances and oxygenation improved, blood lactate levels were reduced and SOFA score got slightly better. These results were maintained at least 12 hours after the endotoxin removal treatment completion. Evolution of clinical parameters are summarized in Table 1.
No device failure or adverse events occurred during treatments. The patient was still alive 28 days after the Alteco LPS Adsorber treatment and his total ICU stay was 47 days.
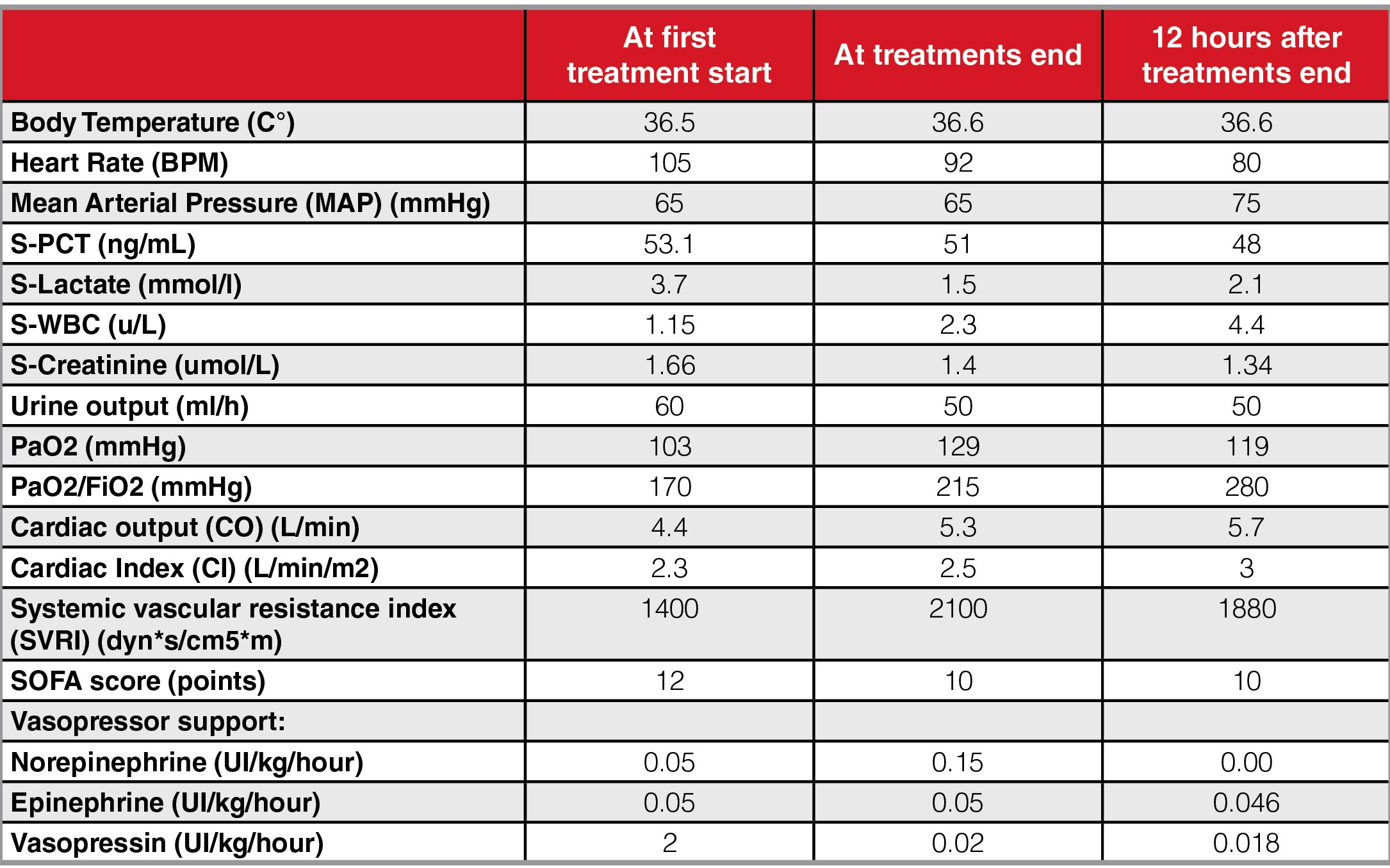
Table 1
Discussion
Our single clinical experience shows the potential role of endotoxin removal in septic shock. This may indicate removing endotoxin from the bloodstream could play a role as an additional therapy in order to gain time for the etiological therapies to work. Further clinical investigation is needed to determine role and effectiveness of LPS adsorption in endotoxemic shock.
Conclusion
This clinical report of treatment with Alteco LPS Adsorber in endotoxemic septic shock from pyelonephritis, caused by the gram-negative bacteria E. Coli, shows that the treatment was safe and hemodynamic and respiratory variables improved.

Endotoxin removal
The Alteco LPS Adsorber contains discs made of porous polyethylene (PE) covered in a tailor-made peptide. The peptide binds to lipid A (the toxic part of endotoxin) with high affinity. By adsorbing harmful levels of endotoxin from the patient’s bloodstream, the Alteco LPS Adsorber can break the chain of immune system overreactions that can spiral into septic shock. This helps to stabilize the patient’s hemodynamic parameters in the acute situation.
1 John C. Marshall, Debra Foster, Jean-Louis Vincent, Deborah J. Cook, Jonathan Cohen, R. Phillip Dellinger, Steven Opal, Edward Abraham, Stephen J. Brett, Terry Smith, Sangeeta Mehta, Anastasia Derzko, Diagnostic and Prognostic Implications of Endotoxemia in Critical Illness: Results of the MEDIC Study, The Journal of Infectious Diseases, Volume 190, Issue 3, 1 August 2004, Pages 527–534, https://doi.org/10.1086/422254
2 Cohen J. (2002). The immunopathogenesis of sepsis. Nature, 420(6917), 885–891. https://doi.org/10.1038/nature01326
3 Rudd, K. E., Johnson, S. C., Agesa, K. M., Shackelford, K. A., Tsoi, D., Kievlan, D. R., Colombara, D. V., Ikuta, K. S., Kissoon, N., Finfer, S., Fleischmann-Struzek, C., Machado, F. R., Reinhart, K. K., Rowan, K., Seymour, C. W., Watson, R. S., West, T. E., Marinho, F., Hay, S. I., Lozano, R., … Naghavi, M. (2020). Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet (London, England), 395(10219), 200–211. https://doi.org/10.1016/S0140-6736(19)32989-7
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(19)32989-7/fulltext
4 Global report on the epidemiology and burden of sepsis: current evidence, identifying gaps and future directions. Geneva: World Health Organization; 2020. Licence: CC BY-NC-SA 3.0 IGO.
5 Zhang, J., Ankawi, G., Sun, J., Digvijay, K., Yin, Y., Rosner, M. H., & Ronco, C. (2018). Gut-kidney crosstalk in septic acute kidney injury. Critical care (London, England), 22(1), 117. https://doi.org/10.1186/s13054-018-2040-y
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5934860/
